

🕐 Read Time: 16 min
Cardiology EHR with Integrated Billing and Coding
Cardiology practices operate in one of the most billing-intensive environments in outpatient medicine. A single patient visit can generate multiple billable events, an office evaluation, an echocardiogram interpretation, a stress test reading, and a telehealth follow-up, each carrying its own CPT code, modifier, and payer rule. One documentation gap, one wrong modifier, or one missed prior authorization is enough to trigger a denied claim, delay a payment, or create a compliance exposure.
Many cardiology clinics still manage billing and clinical documentation through separate systems. A clinician documents in the EHR. A coder reviews a printout. A biller re-enters data into a standalone billing platform. A front desk employee handles eligibility checks manually. This disconnected approach creates friction at every handoff. Errors compound. Administrative workload grows. Revenue leaks at multiple points in the cycle.
A cardiology EHR with integrated billing and coding addresses this problem by connecting clinical documentation, coding logic, claim creation, and payment processing inside a single platform. When the system works as designed, the workflow becomes faster, more accurate, and easier to manage, particularly for small and independent cardiology practices that cannot sustain a large administrative team.
This article explains how integrated billing and coding works inside a cardiology EHR, which features matter most, how to evaluate the right system, and what practices typically experience when they make the transition. For a broader look at how EHR selection affects cardiology operations, see what US practices are getting wrong about cardiology EHR in 2026.
What Is a Cardiology EHR with Integrated Billing and Coding
A cardiology EHR with integrated billing and coding is a software platform that combines clinical documentation, medical coding, insurance claims management, and payment processing into one connected system. Rather than requiring separate tools for each function, the integrated platform shares data across all workflows automatically, eliminating the manual handoffs that create errors in disconnected environments.
In a traditional setup, the clinical and billing sides of a practice operate in separate lanes. A cardiologist documents an encounter. The note is exported or printed. A coder assigns ICD-10 and CPT codes manually. A biller enters those codes into a billing platform and submits the claim through a clearinghouse. Any error at any stage requires a manual correction that adds time and delays payment.
In an integrated system, this entire sequence happens within a single interface. The EHR captures clinical documentation, suggests codes based on the documented diagnosis and procedure, builds the claim automatically, checks it for errors, and routes it for electronic submission. The clinician, coder, and biller all work within the same platform without re-entering data at any point.
For a detailed comparison of how leading platforms handle this integration, the top 5 cardiology EHR systems for US practices in 2026 breaks down each platform’s billing capabilities side by side.
What integrated billing and coding typically includes:
- Clinical documentation linked directly to billing events
- Automated ICD-10 and CPT code suggestions based on structured clinical notes
- Real-time insurance eligibility verification before or at the point of service
- Claim creation and scrubbing before submission
- Electronic claim submission through a clearinghouse integration
- Remittance processing and automated payment posting
- Denial tracking and resubmission workflows
The depth of integration varies significantly by platform. Some systems offer tight native integration across all functions. Others connect billing through third-party modules that require periodic data syncing. Understanding that distinction is critical when evaluating a cardiology EHR system for billing use, because loosely coupled integrations can reproduce many of the same data-entry problems that disconnected systems create.
Why Billing and Coding Are Critical for Cardiology Clinics
Cardiology billing is more complex than billing in most primary care or general specialty settings. The volume and variety of billable services is higher, payer rules are more specific, and the margin for coding error is narrower. According to CMS guidelines for cardiology billing, cardiology procedures carry some of the highest reimbursement values in outpatient medicine — which also means the financial impact of a denied or downcoded claim is proportionally greater.
High Volume of Procedure Codes
A cardiologist may perform or interpret echocardiograms (CPT 93306, 93307, 93308), nuclear stress tests (CPT 78451 through 78454), Holter monitor readings (CPT 93224, 93226), cardiac catheterizations (CPT 93454 through 93461), device checks for pacemakers and implantable cardioverter-defibrillators, and multiple levels of evaluation and management (E/M) services across a single patient panel. Each procedure requires a specific code, and many require modifiers to reflect laterality, technical versus professional component, or supervision level.
Modifier Complexity
Cardiology frequently requires CPT modifiers including 26 (professional component), TC (technical component), 59 (distinct procedural service), and 25 (significant, separately identifiable E/M service on the same day as a procedure). Incorrect modifier use is one of the leading causes of cardiology claim denials and reimbursement downgrades. The American College of Cardiology publishes updated coding guidance annually that reflects these modifier requirements in detail.
Payer-Specific Rules
Medicare, Medicaid, and commercial payers each apply different Local Coverage Determinations (LCDs) for cardiology procedures. Prior authorization requirements, bundling rules, and frequency limitations differ by payer and by procedure. A claim that is valid for one payer may be denied by another based on coverage policy differences that are invisible to a billing team using a generic system without specialty-specific payer logic built in.
High Reimbursement Stakes
Cardiology procedures carry higher reimbursement values compared to many other specialties. An echocardiogram with Doppler and color flow mapping reimburses several hundred dollars under Medicare. A denied claim represents a meaningful revenue loss, particularly for small practices that operate on tight monthly cash flow. Research from the Medical Group Management Association (MGMA) consistently shows that practices with high denial rates spend disproportionate staff time on rework, time that could otherwise be directed at patient care.
Documentation Burden
Cardiology notes must be thorough to support the level of service billed. For a high-complexity E/M visit, the clinical note must reflect medical decision-making of sufficient complexity. Incomplete documentation leads to coding downgrades that directly reduce reimbursement. This is a challenge the best cardiology EHR software addresses through structured documentation that guides clinicians to capture the required elements at the point of care.

How Billing and Coding Integration Works in an EHR
Understanding the mechanics of integration helps practices assess whether a platform will actually reduce administrative burden or simply shift it to a different screen. Here is how a well-integrated cardiology EHR handles each phase of the billing cycle.
Phase 1: Clinical Documentation
The billing process begins at the point of documentation. When a cardiologist documents an office visit, procedure, or test interpretation, the EHR captures structured data, diagnosis codes, procedure descriptions, clinical findings, and the time and context of service. In systems with AI-Powered Documentation capabilities, the clinical note can be generated from voice input or ambient conversation capture, reducing documentation time while preserving the detail needed to support accurate coding.
The more structured the documentation, the more reliably the system can suggest billing codes. Structured note templates designed for cardiology, covering chest pain evaluations, arrhythmia workups, post-procedure follow-ups, and device management visits, make the coding step faster and more consistent. For a deeper look at how AI documentation is changing cardiology workflows, see the guide to AI EHR for cardiology.
Phase 2: Coding
Once documentation is complete, the integrated EHR uses the captured clinical data to suggest ICD-10 diagnosis codes and CPT procedure codes. In advanced systems, this is handled through Auto Capture of ICD and CPT Codes that map documented findings to standard code sets without requiring a coder to search manually.
The coding engine typically flags missing codes for documented procedures, potential upcoding or downcoding based on documentation detail, code combinations that payers commonly bundle or deny, and required modifiers that the billing team needs to apply.
Human review remains important, particularly for complex encounters. In most cardiology clinics, a certified coder or billing specialist reviews system-generated codes before claim submission. Integration reduces the time spent searching manually but does not replace professional coding judgment.
Phase 3: Claim Creation
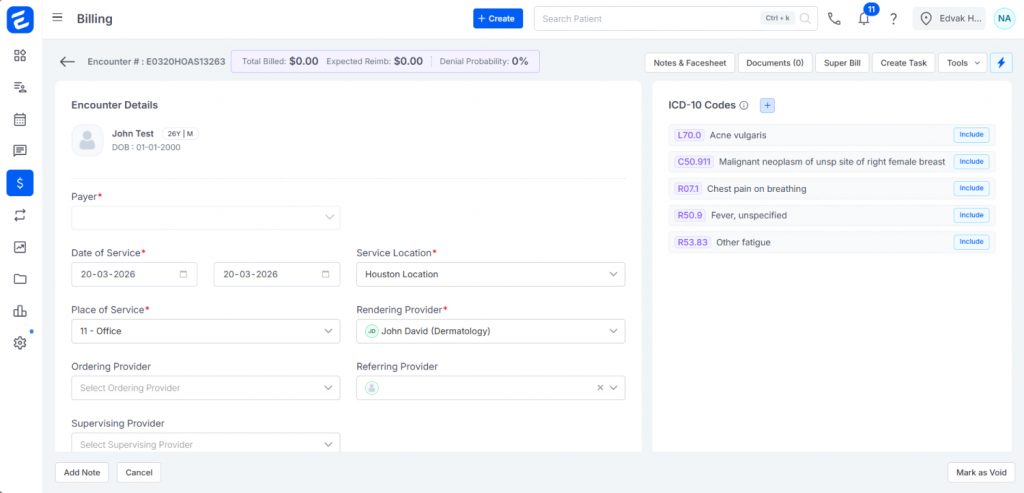
After codes are confirmed, the EHR builds a CMS-1500 or electronic 837P claim file. The claim pulls patient demographics, insurance information, provider NPI numbers, referring provider data, and diagnosis and procedure codes from the same system. This eliminates transcription errors that occur when billing staff re-enter data from a clinical system into a separate billing tool.
Built-in claim scrubbing reviews each claim against payer rules, CMS edits, and internal coding logic before submission. Common errors caught at this stage include unbundled codes, missing modifiers, invalid diagnosis-to-procedure code combinations, date of service discrepancies, and authorization numbers not attached to the claim.
Phase 4: Submission
Clean claims are submitted electronically to the appropriate insurance payer through a clearinghouse integration. The EHR tracks claim status in real time, updating the billing team as claims are accepted, rejected, or pended. Claims Management tools within the platform allow billing staff to see the full status of every outstanding claim without logging into a separate payer portal. For practices evaluating how this works across different systems, the cardiology billing solutions guide covers the submission workflow in detail.
Phase 5: Payment and Reconciliation
When payers process claims, electronic remittance advice (ERA) files are returned. The integrated EHR reads these files and posts payments automatically to the correct patient accounts and service lines. Adjustments, write-offs, and patient balances are calculated and recorded. Staff can review posted payments, identify underpayments, and initiate appeals directly within the system through Payment Processing tools built into the platform.
Key Features of an Integrated Cardiology EHR System
Not all EHR systems offer the same depth of billing integration. These are the features that matter most for a cardiology-specific billing workflow. For a full feature-by-feature breakdown across leading platforms, the best cardiology EHR for small clinics in 2026 covers this in detail for independent and small group practices.
ICD-10 and CPT Code Automation
The system should suggest accurate cardiology-specific codes based on structured clinical documentation. The code library should be updated annually to reflect CMS code set changes published each October. In well-designed integrated systems, codes are suggested contextually based on the specialty template used for documentation rather than requiring the coder to search a generic code list.
Real-Time Insurance Eligibility Verification
Eligibility verification should occur before or at the time of service, not after a claim is denied. Real-Time Insurance Eligibility Checks allow front desk staff to confirm a patient’s coverage status, copay, deductible, and authorization requirements within seconds of scheduling or check-in. This prevents claims from being submitted for patients with lapsed, terminated, or incorrectly recorded insurance coverage.
Claims Scrubbing and Error Detection
A built-in claim scrubber reviews each claim against payer-specific rules, CMS edits, and internal coding logic before submission. Common cardiology-specific errors caught at this stage include unbundled echocardiography component codes, missing stress test modifiers, invalid diagnosis-to-procedure pairings, and missing authorization reference numbers.
Prior Authorization Tracking
Many cardiology procedures require prior authorization, including nuclear stress tests, echocardiograms for certain indications, and most cardiac imaging studies. According to the American College of Cardiology’s advocacy resources, prior authorization burdens in cardiology are among the highest of any specialty. An integrated EHR should track authorization status by patient and procedure, alert staff when authorization is pending or expired, and flag encounters where the authorized procedure does not match the service documented and billed.
Denial Management and Resubmission
When claims are denied, the system should capture the denial reason code, categorize denials by type, and route them to the appropriate staff member for resolution. The ability to track denial trends over time helps practices identify recurring errors and correct them at the source.
Reporting and Revenue Analytics
The EHR should provide accessible reports on claim submission rates, denial rates by payer and code, days in accounts receivable, collection rates, and revenue by provider or service type. Analytics and Reporting tools that surface these metrics allow practice administrators to monitor and improve billing performance without relying on a separate revenue cycle management service.
Benefits of Integrated Billing and Coding
The benefits of EHR billing integration are well documented across specialty practices. For cardiology specifically, the impact is amplified because of the complexity and volume of billable services per patient visit.
Faster Claim Submission
In most cardiology clinics using disconnected systems, the lag between service and submission ranges from three to seven days due to documentation review, manual coding, and data re-entry. Integrated systems reduce this to one to two days in typical workflows. The cardiology EHR implementation guide covers what practices should expect during the transition to an integrated billing workflow.
Fewer Coding Errors
Manual coding from clinical notes introduces human error at multiple points. Automated code suggestions based on structured documentation reduce these errors, particularly for high-frequency, high-value cardiology procedures where coding precision directly affects reimbursement.
Reduced Claim Denials
Each denied claim requires staff time to investigate, correct, and resubmit, with no guarantee of eventual payment. By catching errors before submission through claim scrubbing, verifying eligibility at the front end, and applying payer-specific rules during claim creation, integrated systems reduce the volume of denials before they reach the billing team. This is explored in depth in the cardiology medical billing solutions guide.
Improved Cash Flow
Faster submission, fewer denials, and automated payment posting all contribute to a shorter revenue cycle. For small cardiology practices with limited operating reserves, even a five to ten day improvement in average payment timing can have a meaningful impact on monthly liquidity.
Reduced Administrative Workload
Integration removes manual steps from the billing process. This allows a small billing team to manage a higher claim volume without adding headcount, particularly relevant for independent cardiology practices where administrative staff handle multiple roles simultaneously.
Stronger Compliance Posture
When documentation and coding are connected inside the same platform, there is an auditable trail linking each billed code to the clinical note that supports it. This reduces exposure in the event of a payer audit or a Medicare Recovery Audit Contractor (RAC) review.

Common Billing and Coding Challenges in Cardiology Clinics
Undercoding Due to Incomplete Documentation
One of the most common sources of revenue loss in cardiology is undercoding, where a clinician documents a high-complexity visit but the note does not contain sufficient detail to support billing at a higher E/M level. The coder downcodes to avoid a compliance risk, and the practice collects less than it is entitled to.
Procedure Bundling Errors
CMS and commercial payers bundle certain procedure codes, meaning they will not reimburse them separately when billed on the same date of service for the same patient. CMS’s National Correct Coding Initiative (NCCI) edits define which code combinations are subject to bundling. An integrated system with updated NCCI bundling logic catches these before submission rather than after denial.
Authorization Gaps
Cardiology procedures that require prior authorization generate a significant share of denials when authorization is not obtained, when it expires before the service date, or when the authorized procedure does not match the service actually performed.
Global Period Billing Conflicts
When a cardiologist performs a procedure, a global period applies during which most follow-up services are included in the procedure reimbursement and cannot be billed separately. Billing an E/M visit during the global period without modifier 24 results in a claim denial. CMS global surgery billing rules define these periods for each procedure code.
Payer Rule Variability
Different payers apply different LCDs for cardiology procedures. Billing staff in small practices often lack the bandwidth to track payer-specific rule changes, leading to denials that could have been avoided with better system-level payer rule logic.
How Integrated EHR Systems Reduce Claim Denials
Research from MGMA consistently finds that practices with high denial rates spend disproportionate staff time on rework. An integrated cardiology EHR addresses denial risk at multiple points in the claim lifecycle rather than treating denial management as a downstream clean-up function.
Pre-Visit Eligibility Checks
Most eligibility-related denials occur because a practice submitted a claim without confirming that the patient was covered under the insurance on file at the time of service. Integrated systems run eligibility checks at scheduling or check-in, flagging coverage issues before the patient is seen.
Real-Time Claim Scrubbing
Before a claim leaves the practice, integrated systems run it through editing rules based on CMS guidelines, payer contracts, and common coding policies. Claims that fail the scrub are returned to the billing team with specific error codes and suggested corrections.
Automated Coding Suggestions
Coding errors are a leading cause of cardiology claim denials. Automated coding suggestions based on structured clinical data reduce the frequency of these errors by aligning what the clinician documents with what the system recommends for billing.
Denial Pattern Analysis
Integrated systems with reporting tools allow billing teams to analyze denial patterns over time. If a specific payer consistently denies a particular procedure code, the system data makes those patterns visible. Practices can investigate the root cause and correct it before it compounds. The cardiology EHR pricing guide for 2026 also covers how denial reduction impacts the total cost of ownership of an integrated platform versus standalone tools.
Step-by-Step Cardiology Billing Workflow Using EHR
Step 1: Schedule and Eligibility Check
When a patient is scheduled, the EHR triggers an automated insurance eligibility check. The system confirms the patient’s coverage, copay amount, deductible status, and any authorization requirements for the planned service.
Step 2: Check-In and Demographic Verification
At check-in, the front desk verifies patient demographics and insurance information. Using Scheduling tools integrated with the billing system, staff can see outstanding balances, active authorization numbers, and any prior claim issues associated with the patient account.
Step 3: Clinical Documentation
The cardiologist documents the encounter using structured cardiology templates. In systems with AI-Powered Documentation or Integrated Speech-to-Text capabilities, voice dictation or ambient capture tools generate the structured note from the clinical encounter, reducing documentation time without sacrificing the detail required for accurate coding. For practices considering switching platforms to access these capabilities, the cardiology EHR data migration guide covers what to expect during the transition.
Step 4: Code Assignment
Based on the completed documentation, the EHR suggests ICD-10 and CPT codes. A certified coder or billing specialist reviews the suggestions, adds modifiers where needed, and approves the encounter for billing.
Step 5: Claim Creation and Scrubbing
The EHR builds the claim automatically using confirmed codes, patient demographics, provider information, and insurance data already in the system. The built-in scrubber checks the claim against payer rules and CMS editing logic.
Step 6: Electronic Submission
Clean claims are submitted electronically through the integrated clearinghouse. The EHR updates claim status in real time across the entire claim portfolio.
Step 7: Payment Posting and Reconciliation
When the payer processes the claim, an ERA file is returned. The EHR reads the ERA and posts payments, adjustments, and write-offs automatically to the correct service lines.
Step 8: Denial Management
Denied claims are captured by the system and categorized by denial reason code. The billing team receives a prioritized worklist with the denial explanation and suggested next steps.
How to Choose the Right Cardiology EHR with Billing
Depth of Native Billing Integration
Ask specifically whether billing is native to the platform or connected through a third-party module. For a structured framework to evaluate this, the cardiology EHR implementation guide includes a vendor evaluation checklist built specifically for billing integration assessment.
Cardiology-Specific Code Libraries and Templates
Confirm that the platform includes the full range of cardiology CPT codes, structured documentation templates for common cardiology encounter types, and annual code set updates aligned with CMS’s annual Physician Fee Schedule updates.
Claim Scrubbing Quality
Ask vendors to describe how their claim scrubber works and which rule sets it applies. The most effective scrubbers apply multiple editing layers simultaneously, CMS edits, payer contract rules, and specialty-specific coding logi, before a claim leaves the practice.
Reporting and Denial Tracking
The system should surface denial rates by payer and code, days in accounts receivable, collection rates, and revenue by provider or service type. Benchmarking your denial rates against MGMA’s performance data helps identify whether your rates are above or below industry averages for cardiology practices.
Implementation and Training Support
Billing system transitions are operationally disruptive. The cardiology EHR implementation process guide covers realistic timelines and what support to expect from vendors during the go-live period.
Total Cost of Ownership
Compare the total cost of an integrated platform against the combined cost of the separate systems it would replace. The cardiology EHR pricing guide provides a detailed breakdown of cost structures across different platform types, including per-provider pricing, module fees, and clearinghouse transaction costs.
Why Edvak Is a Strong Option for Cardiology Billing Integration
For small and independent cardiology clinics evaluating an integrated EHR, Edvak offers a platform built around specialty-specific workflows rather than adapted from a primary care template. The best EHR for cardiology guide covers how Edvak compares to general-purpose platforms across documentation, billing, and practice management functions.
The Advanced EHR includes structured documentation templates for cardiology encounters, voice and AI documentation support through tools like Conversation Capture to Structured Notes, and electronic lab and imaging integration that connects diagnostic results directly to clinical notes — ensuring the documentation needed to support billing is captured at the point of care.
The Billing and Revenue Cycle Management module connects directly to the clinical EHR and covers real-time eligibility verification, automated code capture, claim scrubbing, electronic submission, ERA processing, and denial management within a unified workflow.
The Practice Management layer ties scheduling, patient registration, and front desk workflows to the billing system, so eligibility checks, authorization tracking, and patient balance collection become part of the pre-visit process rather than a reactive correction after a denial.
Analytics and Reporting tools give practice administrators visibility into denial trends, collection rates, and revenue cycle performance without requiring a third-party analytics service.
For state-specific considerations, Edvak has published dedicated guides for practices in California, Texas, and New York that cover the payer mix, regulatory environment, and operational pressures unique to each market. Follow Edvak’s ongoing cardiology content updates on LinkedIn for the latest insights on EHR selection, billing optimization, and practice management for US cardiology clinics.
Frequently Asked Questions for Cardiology EHR with billing and coding
-
1. What does integrated billing mean in a cardiology EHR?
Integrated billing means clinical documentation, coding, claim creation, submission, and payment posting are handled within the same platform rather than across separate systems. The clinical note drives the billing process automatically, eliminating manual data re-entry between systems and reducing the errors that result from it. CMS's overview of electronic health records and billing provides useful context on what payers expect from integrated documentation and billing workflows.
-
2. How does EHR improve billing accuracy in cardiology?
An integrated EHR improves billing accuracy by using structured clinical documentation to suggest diagnosis and procedure codes, applying claim scrubbing logic before submission, verifying eligibility before the patient visit, and tracking prior authorizations across the patient panel. Each step removes a category of error that would otherwise surface as a denied or downgraded claim.
-
3. What is ICD and CPT automation in a cardiology EHR?
ICD and CPT automation refers to the system's ability to suggest standard billing codes based on what the clinician documents in the clinical note. ICD-10 codes identify the diagnosis being treated. CPT codes identify the specific procedure or service performed. The American Medical Association maintains the CPT code set and publishes annual updates that integrated EHR systems incorporate into their coding engines.
-
4. Can EHR reduce claim denials in a cardiology practice?
Yes, in most cases. Integrated EHR systems reduce denials through pre-visit eligibility verification, real-time claim scrubbing before submission, automated coding suggestions, and denial tracking tools that identify patterns over time. The degree of denial reduction depends on the depth of the platform's billing integration and how consistently staff use the system's workflow tools.
-
5. How does billing integration improve revenue for cardiology clinics?
Billing integration improves revenue by shortening the time between service and payment, reducing denied claims, catching undercoding before claims are submitted, and enabling faster identification of underpayments that can be appealed. The cardiology medical billing solutions guide covers the revenue impact in detail with specific examples from cardiology billing workflows.
-
6. Is standalone billing software better than an integrated cardiology EHR?
In most practice environments, a well-integrated cardiology EHR outperforms a standalone billing system because clinical and billing data share the same platform and do not require manual transfer or synchronization. The data-entry overhead and error risk that come with maintaining a separate clinical system typically offset any advantage a standalone billing tool may offer in specialized billing logic.
-
7. How long does billing setup take in a cardiology EHR?
Implementation timelines vary based on practice size, data migration complexity, and vendor support quality. In most small cardiology clinic deployments, billing setup takes between four and twelve weeks. The cardiology EHR implementation guide covers the full timeline in detail, including what to expect at each phase from data migration through go-live.
Ready to take the next step?
Get a personalized demo and see how Edvak can drive real impact to your practice.
Related Blogs



More Categories
Edvak.com Terms & Conditions Privacy Policy © 2026 Edvak. All rights reserved.